
Teledermatology: why dermatology is uniquely suited for asynchronous care
This article gives you an overview of what teledermatology is, and how you can get started offering online consultations to your patients via Miiskin.

Table of Content
What is teledermatology? | Why organizations are adopting it? | Key benefits | Types of teledermatology | Which model works best for enterprise | Teledermatology applications | Miiskin a teledermatology platform | FAQ
Dermatology is one of the few medical specialties where a large proportion of clinical decisions can be made using images and structured patient information. This makes it uniquely suited to asynchronous care and positions teledermatology as a powerful tool for expanding access to specialist expertise.
While telehealth has transformed many areas of healthcare, dermatology stands apart. Because skin conditions are primarily visual, asynchronous teledermatology allows specialists to review and manage cases efficiently without requiring real-time appointments. For health systems, insurers, and dermatology organizations, this creates an opportunity to increase access to care without proportionally increasing specialist capacity.
Partner with Miiskin
Miiskin works with health systems and HMOs to deliver scalable dermatology care through a HIPAA-compliant teledermatology platform.

What is Teledermatology?
Teledermatology is a form of telemedicine that enables dermatologists to assess, diagnose, and manage skin conditions remotely using digital images and patient-submitted clinical information.
For health systems, HMOs, and dermatology chains, teledermatology is not just a convenience—it is a way to extend specialist capacity, improve access to care, and optimize resource allocation across large patient populations and multiple locations.
Why organizations are adopting teledermatology
The adoption of teledermatology is driven by a combination of clinical, operational, and financial factors:
- Rising demand for dermatology services and limited specialist availability
- Long wait times for in-person consultations
- Uneven access across regions and populations
- Operational inefficiencies in traditional care delivery models
Teledermatology helps address these challenges by enabling faster triage, reducing unnecessary in-person visits, and allowing dermatologists to manage more patients within the same timeframe.
Key benefits of teledermatology for health systems and dermatology chains
- Improved access to care: Organizations can expand dermatology services to underserved regions and reduce patient wait times.
- Increased specialist efficiency: Asynchronous workflows allow dermatologists to review cases on their own schedule, increasing throughput.
- Reduced operational costs: Fewer in-person visits and more efficient workflows lower the cost of care delivery.
- Better patient outcomes: Faster diagnosis and treatment initiation improve clinical outcomes and patient satisfaction.
- Scalable care delivery: Teledermatology enables organizations to grow services without proportional increases in staffing.
What are the types of Teledermatology?
Store-and-forward (Asynchronous) Teledermatology
Store-and-forward teledermatology is the most commonly used modality. It involves capturing high-quality clinical images of a patient’s skin condition, along with relevant medical history, and sending them to a dermatologist for review at a later time. This method does not require the patient and dermatologist to be present simultaneously, making it highly flexible and efficient. It is particularly well-suited for routine consultations, follow-ups, triaging cases, or remote areas where immediate specialist access may be limited.
Real-time (Synchronous) Teledermatology
Real-time teledermatology uses live video conferencing to connect patients and dermatologists for face-to-face consultations in real time. This interactive approach allows dermatologists to ask questions, examine the skin visually, and provide immediate feedback or treatment recommendations. While it requires both parties to be available simultaneously and relies on stable internet connectivity, it can be useful for complex cases, when a dynamic discussion is needed, for example when Accutane is being prescribed for severe acne.
Hybrid Teledermatology
Hybrid teledermatology combines elements of both store-and-forward and real-time methods. Typically, patients first send images and information about their symptoms to the dermatologist, who reviews the material before a scheduled video consultation. This model enables dermatologists to prepare in advance and conduct more informed and focused live consultations. Hybrid approaches offer a balance between convenience and interactivity, making them ideal for comprehensive evaluations that require both image review and direct patient engagement.
Mobile Teledermatology
Mobile teledermatology refers to the use of smartphones and smartphone apps for dermatology to deliver care. Although it can support both asynchronous and synchronous interactions, it is often highlighted separately due to its unique advantages and widespread accessibility. Patients can capture and send images, join video calls, or use mobile apps to connect with dermatologists—often with little more than a cellular data connection. Mobile teledermatology is especially valuable in rural, underserved, or low-resource settings where traditional telemedicine infrastructure may be lacking.
Which model works best for large organizations?
For health systems, HMOs, and dermatology chains, asynchronous teledermatology is typically the most effective model.
It allows organizations to:
- Maximize dermatologist productivity
- Reduce scheduling constraints
- Handle higher patient volumes
- Deliver faster time-to-treatment
Partner with Miiskin
Miiskin works with health systems and HMOs to deliver scalable dermatology care through a HIPAA-compliant teledermatology platform.

Teledermatology applications and functions
Teledermatology is used across a range of healthcare settings and patient populations, and it enables various clinical functions that improve access, efficiency, and continuity of dermatologic care. Understanding both the applications (contexts where teledermatology is used) and the functions (specific tasks it enables) helps clarify its full value in modern healthcare.
1. Clinical diagnosis and management of simple skin diseases
Application:
- Used for evaluating and managing remotely acute or chronic skin diseases such as acne, eczema, psoriasis, among others.
- Supports routine consultations, treatment plans, and disease monitoring.
Functions:
- Virtual consultations
- Online patient triage to determine severity and urgency.
- Virtual prescription renewals based on submitted updates.
- Patient follow-up care for chronic or recurrent conditions.
2. Primary care and specialist referral
Application:
- Primary care providers or nurses capture and send images to dermatologists for expert input.
- Common in general practice or low-resource settings with limited specialist access.
Functions:
- Specialist referral for diagnostic confirmation or management guidance.
- Triage support to prioritize in-person vs. remote management.
- Asynchronous consults for non-urgent dermatologic issues.
3. Rural and underserved area access
Application:
- Expands dermatologic services to geographically isolated or underserved populations.
- Helps overcome barriers like travel distance and shortage of specialists.
Functions:
- Store-and-forward consultations initiated by local clinics or patients.
- Real-time virtual visits when infrastructure allows.
- Education and training for local healthcare workers.
4. Home care and long-term care facilities
Application:
- Used in nursing homes, rehabilitation centers, and home-based care settings.
- Reduces the need to transport patients for routine dermatologic evaluations.
Functions:
- Virtual consultations initiated by caregivers or facility staff.
- Ongoing follow-up care for chronic conditions.
- Prescription renewals and wound or lesion monitoring.
Miiskin
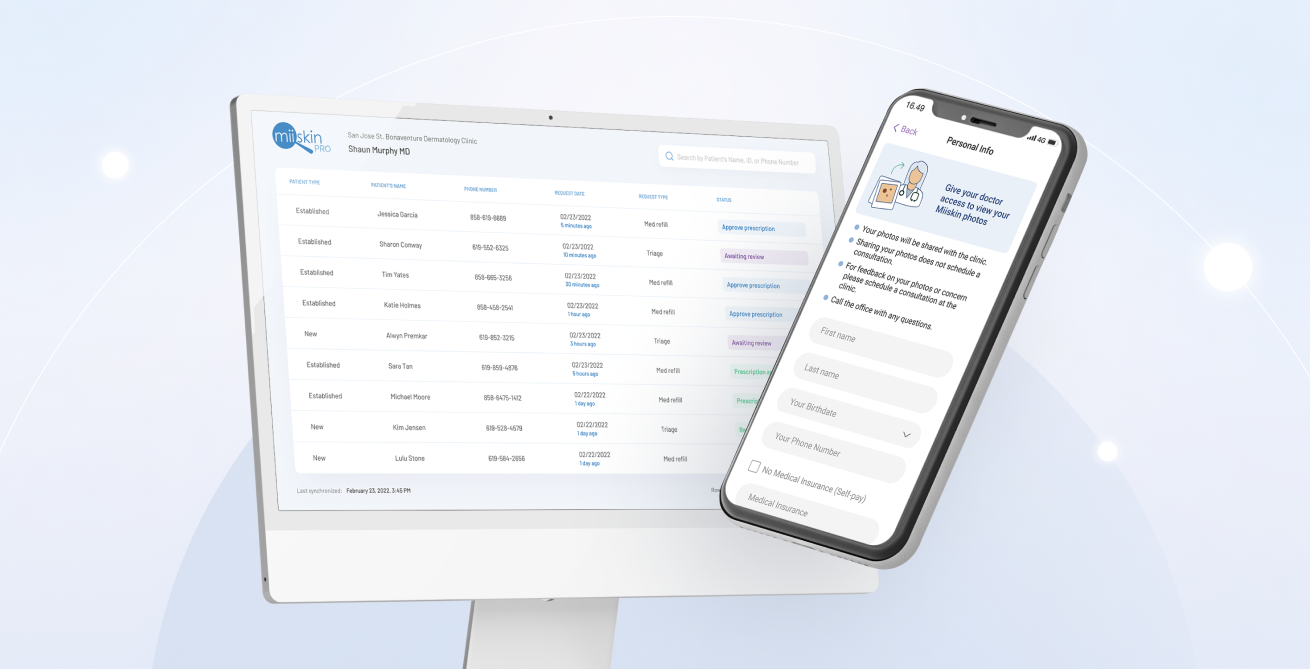
Miiskin is a dermatology-focused teledermatology platform designed to help health systems, HMOs, and dermatology chains deliver scalable, asynchronous skin care services with integrated clinical workflows and prescribing.
Unlike general telehealth solutions, Miiskin is purpose-built for dermatology, enabling efficient image-based consultations, streamlined triage, and longitudinal patient management across distributed care teams and locations.
Why organizations choose Miiskin:
- Asynchronous, high-throughput care delivery: Patients submit images and structured clinical information, allowing dermatologists to review cases and initiate treatment without live consultations—significantly improving provider productivity and reducing wait times.
- Integrated prescribing workflows: Providers can issue prescriptions directly within the platform, connecting diagnosis to treatment in a single workflow and minimizing delays in care delivery.
- Scalable across locations and populations: Organizations can expand dermatology services across regions, clinics, and patient populations without increasing specialist headcount.
- Longitudinal care and follow-ups: Miiskin supports ongoing monitoring of chronic skin conditions through image tracking and structured follow-ups.
- Improved patient experience and adherence: A seamless journey from consultation to prescription improves engagement and treatment adherence.
What organizations can do with Miiskin:
- Deliver teledermatology at scale across multiple locations
- Enable dermatologists to triage, diagnose, and prescribe asynchronously
- Reduce in-person demand and bottlenecks
- Manage chronic dermatologic conditions efficiently
- Improve care coordination across teams
- Streamline clinical and administrative workflows
Best for:
Health systems, HMOs, and dermatology chains looking to expand access, improve efficiency, and scale dermatology services without increasing clinical workload.
Ready to implement teledermatology at scale?
Choosing the right teledermatology platform is a critical decision for health systems, HMOs, and dermatology chains.
To successfully deploy and scale dermatology services, organizations should look for solutions that offer:
- Seamless integration with existing clinical workflows and systems
- Scalability across locations and patient populations
- Intuitive experiences for both patients and care teams
- Support for asynchronous, high-throughput care models
- Integrated prescribing workflows that connect diagnosis to treatment
The right platform doesn’t just enable virtual care—it drives operational efficiency, improves access, and enhances patient outcomes across your organization.
Request a demo to see how Miiskin supports scalable teledermatology across health systems, HMOs, and dermatology chains.
Boost Revenue Growth
Book a demo to learn how.
Partner with Miiskin
Miiskin works with health systems and HMOs to deliver scalable dermatology care through a HIPAA-compliant teledermatology platform.
Frequently asked questions about teledermatology
How effective is teledermatology?
When Teledermatology is conducted by board-certified dermatologists, (like in the case of Miiskin) who have extensive experience in virtual care it is highly effective, particularly for diagnosing and managing common skin conditions. Numerous studies have shown that its diagnostic accuracy is comparable to in-person consultations, especially when high-quality images are provided 1. It improves access to specialist care, reduces wait times, and facilitates timely interventions, especially in remote or underserved areas. While not a replacement for all face-to-face visits, teledermatology is a reliable and efficient tool for many dermatologic needs.
What is the process of teledermatology?
The teledermatology process typically begins with the patient or a referring provider capturing and submitting clinical images of the skin concern along with relevant medical history. These are then reviewed by a dermatologist either asynchronously (store-and-forward) or during a live video consultation (synchronous). After evaluation, the dermatologist provides a diagnosis, treatment plan, or recommendation for further follow-up. Patients receive results and care instructions through the HIPAA-compliant Miiskin platform and patients can write questions and concerns to the dermatologist directly through the platform.
How long do teledermatology results take?
The turnaround time for teledermatology results depends on the dermatologist, but via the Miiskin platform, doctors provide feedback within 24 to 48 hours. For example, Miiskin reports that 90% of online consultations are reviewed by a dermatologist in less than 24 hours, although results may take up to two business days during high-volume periods or holidays.
What happens after teledermatology?
After a teledermatology consultation via Miiskin, the patient typically receives a diagnosis or clinical opinion, along with a treatment plan. This may include starting or adjusting medications, receiving prescriptions, or monitoring the condition at home. If the case is complex or unclear, the dermatologist may recommend an in-person follow-up for further examination, or lab tests. The Miiskin platforms also provides follow-up messaging to ensure treatment effectiveness and address new symptoms.
What is the use of teledermatology?
Teledermatology is used to diagnose, monitor, and manage skin conditions remotely, offering a convenient alternative to in-person visits, often at a more affordable price. It improves access to dermatologic care for patients in rural or underserved areas, facilitates faster triage and referrals, supports chronic condition follow-ups, and allows for efficient prescription management. It’s also valuable in home care settings, long-term care facilities, and hospitals lacking full-time dermatologists.
What are the modalities of teledermatology?
Teledermatology is delivered through three main modalities: store-and-forward (asynchronous), where images and information are submitted and reviewed later; real-time (synchronous), which involves live video consultations; and hybrid models, which combine both approaches. These modalities can be accessed via desktop platforms, mobile apps, or integrated healthcare systems, depending on patient preference and clinical context.
Does insurance cover telemedicine?
Most direct-to-consumer telemedicine platforms, including Miiskin, do not accept insurance. However, their prices are often lower than the out-of-pocket cost of an in-person visit—sometimes even less than a typical specialist co-pay. For example, with Miiskin, you can consult a board-certified dermatologist for just $39 to $59 per visit, without subscriptions or hidden fees. That’s convenient, affordable care—no insurance required.
How much is the average dermatologist visit without insurance?
The average cost of a dermatologist visit without insurance in the U.S. typically ranges from $100 to $250, depending on factors like location, provider fees, and the nature of the visit. For patients paying out-of-pocket, this can be a significant expense. As a more affordable alternative, platforms like Miiskin offer access to board-certified dermatologists for just $39 to $59 per consultation, with no subscriptions or insurance required—making expert skin care more accessible and budget-friendly.
Do doctors like telemedicine?
Yes, many doctors—especially dermatologists—appreciate the flexibility and efficiency that telemedicine offers, particularly through asynchronous platforms like Miiskin. Unlike traditional appointments, asynchronous care allows providers to review cases on their own schedule, whether between appointments, after hours, or from home. With detailed patient questionnaires and high-quality images submitted through the platform, dermatologists have all the information they need to deliver accurate, personalized care—without the pressure of live consultations. This model not only improves work-life balance but also helps doctors serve more patients without sacrificing clinical quality.
Want to learn more about teledermatology?
Check out our articles
Miiskin improves access to high-quality dermatology consultations in the U.S.
8 Top dermatology platforms with integrated prescribing in 2026
Teledermatology: Bridging the gap in dermatological care
Miiskin the future of teledermatology: What four dermatologists learned firsthand
How store and forward telehealth supports direct-to-consumer healthcare
7 Teledermatology apps doctors should know about
5 Teledermatology companies to choose from based on your needs
Choosing the right teledermatology software
 Bring teledermatology to your organization
Bring teledermatology to your organization
Book a Demo →

7 Innovative Tools for Dermatolgists
The 7 advanced dermatology tools to improve healthcare and boost patient experience.
